Pediatric Reconstructive Surgery: Ongoing Treatment Following Major Initial Operation

Pediatric Reconstructive Surgery: Ongoing Treatment Following Major Initial Operation
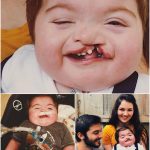
A 3-year-old child who previously underwent a complex 7-hour surgical procedure with a reported 50% survival risk is now preparing for a further major reconstructive operation as part of an ongoing treatment plan.
According to medical context provided, the upcoming procedure will involve mandibular (jaw) reconstruction using autologous rib bone grafting. This type of surgery is typically performed in cases of severe congenital or acquired craniofacial abnormalities where airway function, feeding ability, and facial structure are significantly affected.
The primary goal of the planned intervention is functional improvement rather than cosmetic change. In many pediatric craniofacial cases, reconstruction is aimed at improving airway patency, supporting normal growth, and enabling basic functions such as breathing and eating.
Following her initial surgery, the patient has continued to receive multidisciplinary care, which may include surgical follow-ups, respiratory monitoring, and nutritional support. Pediatric craniofacial reconstruction often requires staged procedures over several years due to growth considerations and the complexity of facial bone development.
 The use of rib grafts in jaw reconstruction is a well-established technique in pediatric surgery, as it allows surgeons to use the patient’s own tissue, reducing the risk of rejection and supporting natural growth integration over time.
The use of rib grafts in jaw reconstruction is a well-established technique in pediatric surgery, as it allows surgeons to use the patient’s own tissue, reducing the risk of rejection and supporting natural growth integration over time.
Despite successful initial intervention, long-term treatment plans for such conditions frequently involve additional surgeries as the child develops. Each stage is carefully timed to balance functional improvement with natural growth patterns.
The patient’s current treatment plan reflects a broader approach in pediatric reconstructive medicine, where the emphasis is placed on improving quality of life outcomes, including airway function, feeding ability, and long-term development.
While the next surgical stage carries inherent risks, it is part of a structured and carefully monitored medical pathway designed to progressively improve essential physiological functions.
Her case illustrates the complexity of early-life reconstructive care and the long-term commitment required from both families and medical teams in managing severe congenital conditions.
Further updates will depend on surgical outcomes and post-operative recovery progress.